Any, even the most minor dental diseases (for example, caries or pulpitis) can lead to serious consequences - the development of osteomyelitis of the jaw with a whole complex of unfavorable symptoms that significantly worsen the general condition and lead to future disability. The disease has multiple causes and risk factors, and the manifestations are specific to various forms. Osteomyelitis of the jaw in the absence of timely treatment may be complicated by pathologies such as meningitis, lung abscess, mediastinitis or encephalitis, which have a high mortality rate (up to 75–90%).
Content
Classification
In modern medicine, there are many options for systematization of osteomyelitis. Depending on the source of infection, there are:
- Odontogenic. It develops as a result of caries or pulpitis. Less commonly, gum disease (gingivitis) is the cause. Through the open areas, pathogenic flora penetrates to the bone tissue and an inflammatory process appears.
- Hematogenous. It is realized by introducing pathogens from any foci of chronic infection (from a simple scratch to chronic cholecystitis).
- Traumatic. It is associated with a direct damaging effect on the jaw bone tissue (punch, gunshot or knife wound, etc.).

Hematogenous osteomyelitis is an inflammation of the bone that develops as a result of the introduction of an infection.
According to the activity of the flow emit:
- Acute (vivid clinical picture, short course);
- Subacute (symptomatology erased, but severe);
- Primary chronic (long-term course with a small number of clinical signs, this group includes atypical forms of osteomyelitis - Garre, Ollier, Brodie abscess, etc.);
- Secondary chronic (develops after the acute one, the duration of the course is from 3 months to 2 years).
According to the etiological characteristic, osteomyelitis of the jaw can be:
- Specific (caused by a specific pathogen, for example, Mycobacterium tuberculosis or pale treponema);
- Nonspecific (caused by a group of any pyogenic bacteria).
Depending on the prevalence of the pathological infectious-inflammatory process, the following forms exist:
- Limited, located in the area of the body, the area is 1–2 teeth;
- Focal, localized in the region of the alveolar process or body of the jaw, but does not exceed the area equal to 3-4 teeth;
- Diffuse (extensive damage of more than 30% of the jawbone).

Forms of the disease in the degree of prevalence
From the point of view of the international classification of diseases (ICD-10), the systematization of osteomyelitis looks like this:
- Acute hematogenous osteomyelitis;
- Other forms of osteomyelitis;
- Subacute osteomyelitis;
- Chronic multifocal osteomyelitis;
- Chronic osteomyelitis with a drained sinus;
- Other forms of chronic osteomyelitis;
- Other osteomyelitis (including Brodie abscess);
- Osteomyelitis of unspecified etiology (also includes bone infection of BDU and periostitis of BDI).
Causes
The influence of many factors provoking the appearance of pathology has been identified and proved. Odontogenic osteomyelitis is the most common (up to 85% of all cases) and is associated with:
- Deep caries;
- Heavy pulp;
- Periodontitis;
- Alveolitis;
- Cystic formations localized in the teeth.
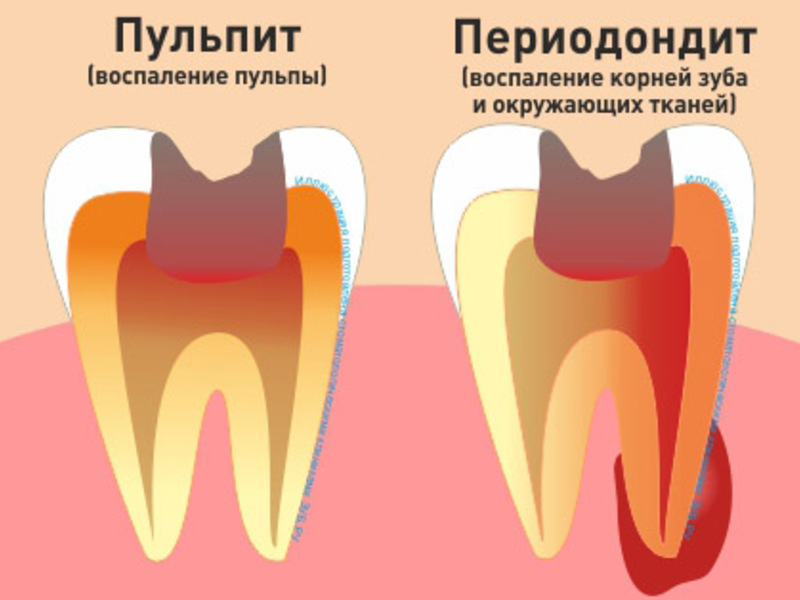
Pulpitis and periodontitis can cause osteomyelitis.
Extremely important conditions for the development of dental inflammation of the bone tissue are infection of the dental pulp and the migration of infectious agents through the neurovascular bundle (the root of the tooth).
With the hematogenous route, any source of infection is the cause. The most frequently distinguished:
- Multiple boils and carbuncles;
- Sepsis caused by any disease (peritonitis, pericarditis);
- Infectious foci in the presence of scarlet fever or diphtheria.
In this way of development, the bone tissue is initially affected, and the teeth are involved for the second time in the absence of adequate and timely treatment of osteomyelitis.
Traumatic form of deviation is about 10% of all cases of the disease. The most common reasons are as follows:
- Fracture of the lower jaw (fracture of the upper jaw practically does not occur);
- Gunshot wounds;
- Stab wounds with periosteum tissue damage;
- Violation of the integrity of the mucous membranes of the nasal cavity.
Most often, the pathogenic flora is represented by the association of various microorganisms and is characterized by the presence of such pathogens as E. coli, Staphylococcus aureus, group B Streptococcus, Klebsiella, Proteus, Pseudomonas aeruginosa and Fusobacteria. Much less often osteomyelitis is caused by a specific microorganism. Such a course is most characteristic of tuberculosis.
At risk are people with diseases accompanied by a decrease in the effectiveness of local and general factors of immune protection. Such conditions cause the following pathologies:
- Diabetes mellitus type I and II;
- Cancer of the blood system (leukemia);
- Rheumatic diseases (polyarthritis, systemic lupus erythematosus, acute rheumatic fever);
- HIV infection;
- Liver and kidney diseases with impaired detoxification and excretory functions.
Clinical picture
The onset of acute osteomyelitis is always sudden (patients call the exact time of onset of clinical signs). The course is characterized by the following symptoms:
- Increased body temperature. From the first hours on the thermometer the mark of 39-40 degrees is recorded. The condition is accompanied by chills and abundant cold, sticky sweat on the entire skin.
- Intoxication syndrome. Patients are lethargic, apathetic, there is general weakness, weakness and a pronounced decrease in appetite. Signs of intoxication are also an increase in heart rate (more than 90 per minute) and a drop in blood pressure.
- Pain syndrome. In odontogenic forms, pain is localized in the region of the causative tooth, radiation to the ear, eye socket, or temple on the affected side is possible. An infected tooth acquires mobility, the mucous membrane of the gums and oral cavity is edematous, hyperemic, ulceration is possible. When hematogenous introduction of pathogens of osteomyelitis, the source of pain is located in the bone tissue itself, there may be no signs of damage from the mucous membranes and teeth. Irradiation is any: from the vertebral bodies (including the lumbar) to any parts of the head.
- Discharge of pus. The masses can be separated from the dental pockets and soft tissues of mucous membranes, in the presence of fistulous passages - from any part of the body (skin of the face, chin, sublingual space, etc.). Discharge has an extremely unpleasant smell of rot.
- Impaired sensitivity. With involvement in the pathological process of the lower jaw, a feeling of tingling, numbness, or crawling from the mucous membrane of the vestibule of the mouth, skin of the chin and lower lip is possible. Symptomatology due to lesions of the branches of the trigeminal nerve.
- Inflammatory infiltration of soft tissues. All neighboring structures are edematous, hyperemic.
Severe edema leads to a significant restriction of the mobility of the lower jaw (when talking or swallowing), difficulty breathing (due to obstruction of the upper respiratory tract). The contours of the face become asymmetrical. Regional lymph nodes are enlarged (they are sharply painful on palpation).

Edema is a characteristic sign of osteomyelitis of the jaw
In case of subacute course, the general condition does not suffer significantly (body temperature does not exceed the level of 37–38 degrees, there are no signs of intoxication). However, the local symptoms of inflammation (edema, pain, impaired function, hyperemia, local temperature increase) are bright and disturb the patient.
It is important! Chronic forms are characterized by a prolonged prolonged course always after acute osteomyelitis. Clinical signs are practically absent.
Occasionally, pain in the primary focus area. The course of the disease can last up to several years. Periodically observed aggravations with severe symptoms. The facial features gradually change, long fistulous passages are formed, from which fragments of bone tissue and pus stand out. Chronic course is always accompanied by pronounced destruction of bone tissue. Multiple decay cavities are formed with small sequestered debris.
Features of the course in children
In young people, the disease has specific features. It always develops extremely rapidly and is accompanied by a septic state. Marked by:
- Convulsions with minor temperature rises (up to 38.5 degrees);
- Dyspeptic disorders due to failure of the central nervous system (nausea, vomiting, epigastric pain, diarrhea stool disorders);
- Significant intoxication (up to coma);
- Changes in behavior and emotional sphere (children are restless, capricious, almost completely refuse to eat, cannot fall asleep without sleeping pills).

In case of signs of disease in children, you should immediately contact a specialist.
Diagnosis of osteomyelitis
During a local examination, the tooth that caused the pathology is mobile and painful with percussion (tapping), teeth loosening and a change in the bite are extremely often observed. The gums adjacent to the tooth tissues are swollen and painful when touched. Enlarged lymph nodes are visualized, they are immobile and painful on palpation.
On external examination, asymmetry of the face, the presence of edema in the area of the lesion extending to the ear, lower and upper eyelid, temple can be expressed.
All patients undergo a complex of laboratory and instrumental examination methods:
- General blood analysis. Against the background of bacterial inflammation, neutrophilic leukocytosis, leukocyte shift to the left, elevated ESR are recorded.
- Biochemical study of blood. On the background of an active inflammatory process, C-reactive protein appears, possibly a violation of protein metabolism (hyperglobulinemia, hypoalbuminemia). With damage to the kidneys and liver (due to intoxication or sepsis), an increase in ALT and AST, alkaline phosphatase, creatinine and urea is possible.
- General urine analysis. Characterized by an increase in erythrocytes, the presence of protein and casts of epithelial cells of the mucous membrane of the renal tubules.
- Sowing discharge from the source of inflammation (bone puncture) on nutrient medium, followed by determination of the pathogen.
- X-ray examination. Although it is a priority, it is carried out only after 1-2 weeks from the onset of the disease (since no signs of pathology are detected in the early stages). By the end of week 1, osteoporosis, a change in trabecular pattern and a decrease in the thickness of the layer of cortical substance are observed. Later, sequestration and fistulous passages can be detected.
- Fistulography - the introduction of a contrast agent (for example, barium sulfate) in fistulous passages followed by x-ray control.Sometimes dyes are used (in children).

Fistulography is one of the methods for diagnosing a disease
Treatment
In most cases, emergency hospitalization is indicated in a surgical or dental hospital.
It is important! Home treatment is unacceptable due to the high incidence of complications caused by inadequate and untimely therapy.
The main goals of treatment are:
- Removal of the source of infection;
- Restoration of the anatomical integrity and functional activity of the jaw.
Drug-free
Diet is indicated only for patients with chronic forms. The diet should be rich in animal proteins (meat of cattle and poultry, eggs, soy proteins), calcium (milk, cottage cheese, cheese, kefir, etc.) and collagen fibers (fruit jelly, aspic).
Also appointed vitamin supplements (vitamins C, D), micro-and macronutrients (calcium, magnesium, phosphorus, fluorine, zinc).
It is important! The substances described are the main components for successful regeneration of bone tissue.
Medicamentous
Conservative therapy is prescribed only for acute osteomyelitis (before the beginning of the formation of cavities of decay) and chronic forms without signs of separation of pus. Showing:
- Broad-spectrum antibiotics. Cephalosporins are prescribed (Ceftriaxone 0.5 to 3 times a day), fluoroquinolones (Ciprofloxacin 0.5 to 2 times a day) or aminoglycosides (Amikacin 15 mg per kilogram of body weight per day). Before obtaining the results of sowing or the impossibility of its conduct, a combination of antimicrobial agents is prescribed, which should cover the entire spectrum of pathogens. If this cannot be done, then Carbopenem or Meropenem are used. The duration of therapy is up to 2 months. Often (with the appearance of chronic forms) repeated courses are shown - 3-5 pieces.
- Nonsteroidal anti-inflammatory drugs. Used to relieve pain. Used "Ibuprofen" (0.4 3 times a day), Ketoprofen (0.1 twice a day). In case of severe pain, it is recommended to give preference to "Ketorolac" (up to 4 tablets (at 0.01) per day) or narcotic drugs ("Morphine", "Promedol").
- Hemostatic therapy. "Etamzilat" 12.5% 5 ml 1 time per day, intravenously or intramuscularly.

Ketorolac is a non-steroidal anti-inflammatory agent.
According to indications, detoxification (intravenous jet infusion of Hemodez or Reopolyglucine solutions), desensitizing (Suprastin, Tavegil) and immunomodulating (human recombinant interferon) therapy is carried out.
In order to reduce the severity of intoxication, hyperbaric oxygen therapy, plasma exchange, and hemosorption can be involved.
It is important! Physiotherapy procedures (ultrasound therapy, UHF, magnetic therapy) have not been used recently, as they have proven to be ineffective.
Surgical
The purpose of the intervention is to remove a purulent-necrotic focus through bone perforation (drilling of holes) at 2–3 points at once and installation in a subsequent drainage. As a result of the elimination of intraosseous elevated pressure, the activity of destruction of viable areas decreases and the severity of pain decreases, the general condition improves.
The rehabilitation of the pathological area is carried out with various solutions (for example, NaCl 0.9% with proteolytic enzymes and antibacterial drugs). Pus and small fragments of bones are quickly removed, areas of bone tissue begin to regenerate.
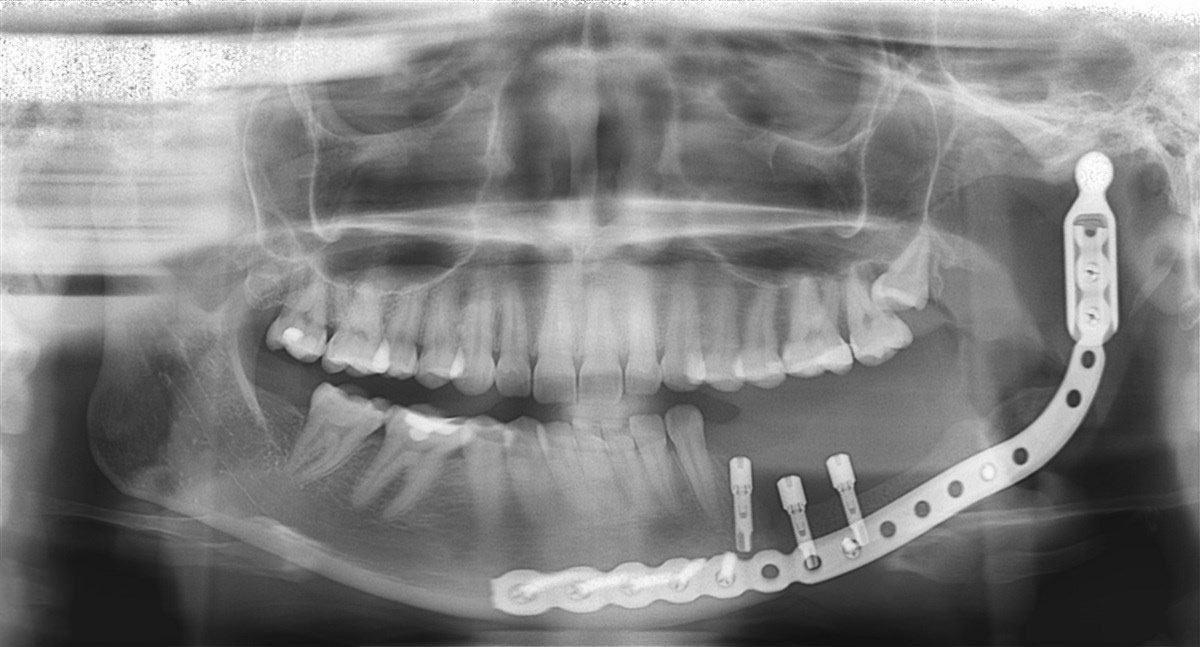
In case of instability of the jaw sections or the threat of fractures, fixation is performed - plates, screws and external structures resembling the Ilizarov apparatus may be involved
When suppuration of the wound, the development of hectic fever or the formation of a fistula shows repeated surgery.
In the postoperative period, a dynamic observation is carried out at the surgeon (at least once every 6 months) with the control radiographs. After 3 months after a complete clinical cure, dental prosthetics are possible.
Complications and prognosis
When rendering untimely or inadequate treatment, the formation of such conditions as:
- Pathological fracture of the jaw. It develops as a result of significant destruction of individual foci and increased load on healthy tissues.
- Soft tissue abscess. It can be located both locally and in distant organs and tissues (with hematogenous or lymphogenous migration of the pathogen). It is a local accumulation of pus, surrounded by a connective tissue capsule.
- Sepsis is the persistence of infectious agents throughout the body with the appearance of many foci of infection in all organs and an inadequate response of the immune system.
- Infectious and toxic shock. Due to the influence on the nerve fibers and vascular walls of a variety of toxins and waste products secreted by bacteria.
- The mandible contracture is a pronounced restriction of the mobility of the anatomical formation with subsequent violations of speech, chewing and swallowing.
- Sinusitis - inflammation of the mucous membrane of the paranasal sinuses.
- Thrombophlebitis of the facial veins - the formation of blood clots (blood clots) in the venous vessels of the face. The affected formations swell, pain and circulatory disorders appear. Possible necrosis of tissues from which the outflow of blood is impaired.
- Mediastinitis - inflammation of the adipose tissue of the mediastinum. It is observed extremely rarely and most often against the background of immunodeficiency states (HIV infection, long-term use of glucocorticosteroids and cytotoxic drugs). Mortality reaches 80%.
It is important! There may be more serious complications (brain or lung abscesses, meningitis, meningoencephalitis), but they are extremely rare (less than 0.001% of all cases). Sometimes develop amyloidosis of the kidneys and heart.
The basis of a favorable prognosis lies in timely access to a doctor, a complete examination of patients and well-chosen treatment. Only a combination of all factors allows for full recovery.
In the absence of therapy, there is a development of complications that quickly lead the patient to disability and disruption of social and labor adaptation.
Prevention
To prevent such a dangerous disease as osteomyelitis, several simple rules should be followed:
- Timely treatment of carious teeth, pulpitis, periodontitis and other dental diseases. The emergence of pain when eating (even sometimes) is already a reason for contacting a specialist.
- Sanation and elimination of any suppurative foci in the body (from furuncle to abscesses in internal organs).
- Enhance local and general immunity. This is facilitated by regular walks in the fresh air, maintaining an active lifestyle (systematic physical activity), giving up bad habits (drinking and drugs, smoking), eating healthy foods.
- Prevention of maxillofacial injuries. If you are prone to fractures, you should avoid dangerous types of work or sports activities.
Video: chronic osteomyelitis
Thus, osteomyelitis is a serious disease that carries a direct threat not only to health, but also to life. When the first symptoms appear, an urgent need to contact a specialist who, after prescribing a set of laboratory and instrumental studies, will make the correct diagnosis and prescribe treatment. The smaller the period of time from the manifestation of osteomyelitis before the start of treatment, the lower the risk of developing complications, including fatal ones.


